From Crisis to Cure: A History of Bone Marrow Transplantation
Welcome to Part 1 of our The Evolution of Cell Therapy series, in which we explore the journey from the first transplant attempts to today’s immune effector cell therapies.
Bone marrow transplantation didn’t start in a lab full of hope; it began in the aftermath of Hiroshima and Nagasaki, where survivors faced catastrophic marrow failure. From early high-risk experiments in the 1950s and 60s to the establishment of global registries and accredited centres, this Insights article traces the journey of BMT from uncertainty and tragedy to a standard, life-saving therapy.

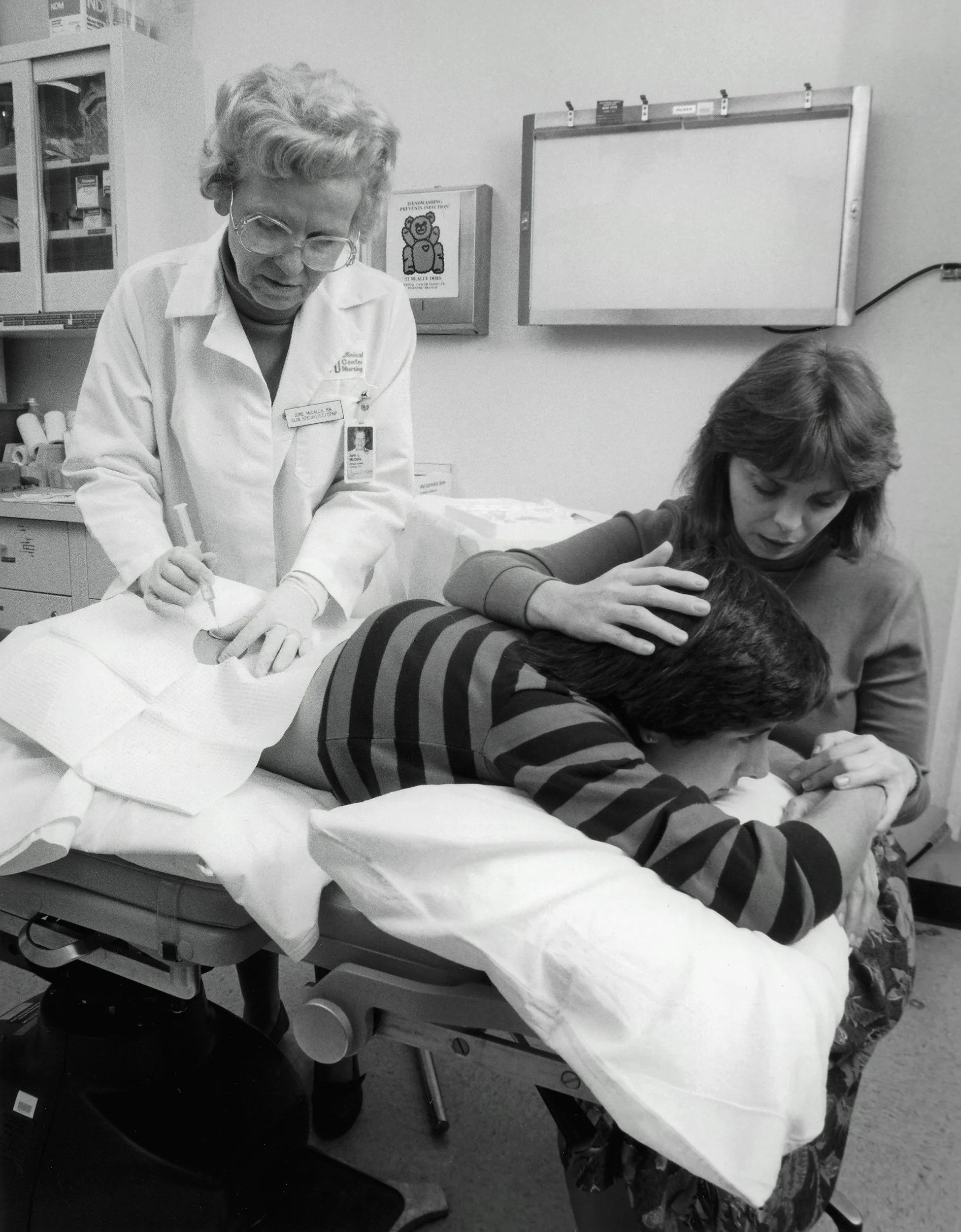
A bone marrow harvest. A large-gauge needle is used to extract the bone marrow, which is transfused into the recipient to help recreate and replenish T-cells, as well as the white and red blood cells killed during chemotherapy. U.S. Navy photo by Photographer’s Mate 2nd Class Chad McNeeley. Public domain, via Wikimedia Commons.
Why BMT Mattered
Bone marrow transplantation (BMT) emerged to tackle some of medicine’s toughest challenges: treating leukaemia and severe genetic immune disorders. In the 1950s, patients with acute leukaemia or congenital immune deficiencies had almost no options. Early scientific breakthroughs, combined with perseverance in the lab and clinic, turned high-risk experiments into a therapy that saves thousands of lives each year [1][2].
Origins in Crisis: Radiation, Stem Cells, and Early Experiments
The atomic bombings of Hiroshima and Nagasaki in 1945 exposed survivors to massive doses of ionising radiation, which selectively destroyed haematopoietic stem cells (HSCs) and progenitors (CMPs, CLPs). Patients suffered pancytopenia, severe infections, bleeding, and often death. Animal studies in irradiated mice and dogs demonstrated that infusing healthy marrow could restore blood production and immune function, providing the mechanistic rationale for human transplantation. [2].
In 1956, E. Donnall Thomas performed the first successful twin-to-twin marrow transplant, proving that haematopoietic reconstitution was possible in humans. Subsequent papers in 1968–69 expanded the approach to children with immune deficiencies, showing partial success but still highlighting challenges like graft-versus-host disease (GVHD) and engraftment failure [1][2].

Diagram showing HSCs, CMPs, CLPs, and their differentiation into blood lineages. Based Mikael Häggström, adapted from A. Rad - Image: Hematopoiesis (human) diagram
out of the dark: ill-fated early human experiments
Researchers experimented with total body irradiation and chemotherapy preconditioning to suppress the immune system and allow donor cells to take. Some patients temporarily recovered neutrophils, platelets, and lymphocytes, but overall outcomes were tragic. Mortimer Bortin, tracking results at the Medical College of Wisconsin, reported 203 deaths by the early 1970s [3]. Each death underscored the steep price of pioneering this life-saving therapy.
UK Milestones: Pioneers and Registries
The UK played a key role in translating these early experiments into routine practice:
1973: First successful unrelated-donor marrow transplant in London.
1974: Anthony Nolan Registry founded after young Anthony Nolan could not find a matching donor. This was the UK’s first systematic approach to connecting patients with unrelated donors, creating a model for global registries [4].
Late 1970s: Great Ormond Street Hospital performed pioneering paediatric transplants, helping establish the UK as a centre for safe, standardised BMT [5].
These developments were crucial in moving BMT from isolated experiments into structured, repeatable clinical practice.
A Personal Tragedy that Changed the Field: Anthony Nolan
Patient stories drove change. Anthony Nolan, born in 1971 with Wiskott-Aldrich syndrome, was too young to survive without a compatible transplant. Despite exhaustive searches, no donor match was found, and he tragically died at age seven. His story was heartbreakingly familiar to clinicians of the time: children with life-threatening blood disorders, and no therapy yet capable of saving them.
In response, Shirley Nolan founded the world’s first unrelated bone marrow donor registry in 1974, aiming to connect patients like Anthony with suitable donors. This registry became a template for international collaboration, laying the groundwork for DKMS (Germany) and the National Marrow Donor Program (US). [4].
Building Global Standards: EBMT and JACIE
By the mid-1970s, it became clear that high-risk procedures needed robust oversight. European pioneers, including Jon van Rood, Bruno Speck, Dick van Bekkum, and Eliane Gluckman, recognised that hope required structure. In 1974, they founded the European Society for Blood and Marrow Transplantation (EBMT), which celebrated its 50th anniversary last year, fostering collaboration, standardising outcomes, and advancing multicentre trials [6][7].
In 1998, JACIE was launched to ensure transplant centres adhered to strict quality and safety standards, covering everything from laboratory handling to chain-of-identity protocols. Over 530 inspections across 25 countries have strengthened reliability in BMT care [8].
The UK Patient and Tissue Pathway
A BMT graft in the UK passes through a defined pathway:
Procurement from donor (bone marrow or peripheral blood).
Processing in accredited labs under HTA licence, ensuring traceability and safety. [9]
Storage in controlled conditions.
Release for transplantation.
Where a graft is used as an Advanced Therapy Medicinal Product (ATMP), MHRA regulation applies. This framework ensures every transplant is safe, traceable, and meets clinical standards. [10] BMT grafts should be processed by a JACIE-accredited centre. Accreditation involves regular, rigorous inspections of laboratory facilities and quality management systems, leading to improved patient survival, reduced complications, and standardised, safer procedures across different countries. [12]
Biovault’s Role Today
Founded in 2002, Biovault Technical operates within this regulated ecosystem. With HTA, JACIE, and MHRA accreditation and full GMP processing capabilities, Biovault supports transplant centres, clinical trials, and NHS partnerships [11]. High-quality processing and traceable storage are essential for patient safety and for enabling cutting-edge therapies derived from bone marrow or other haematopoietic sources.

Into the Light: Modern Bone Marrow Transplantation
Today, haematopoietic stem cell transplantation is a life-saving therapy performed worldwide. In 2023 alone, 47,731 transplants were reported globally, with steadily improving survival rates [10]. What was once grim, uncertain, and experimentally dangerous is now systematic, evidence-driven, and accredited.
References & Further Reading
Nobel Prize in Physiology or Medicine, 1990 – E. Donnall Thomas. https://www.nobelprize.org/prizes/medicine/1990/thomas/lecture/
PMC5101209 – History of PBSC and BMT. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5101209/
Bortin MM. Bone marrow transplantation: a historical perspective. Blood. 1975;45:1–15.
Anthony Nolan Foundation. Our history. https://www.anthonynolan.org
Great Ormond Street Hospital – Early transplant history.
EBMT 50th Anniversary Press Release. Celebrating 50 Years of Community. 2024. https://www.ebmt.org/sites/default/files/2024-03/EBMT-Press-Release-Anniversary-Celebrating%2050%20Years%20of%20Community.pdf
Nature. EBMT turns 50: a milestone in transplantation. 2024. https://www.nature.com/articles/s41409-024-02366-4
JACIE Accreditation History. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK543672/
Human Tissue Authority – Licensing information. https://www.hta.gov.uk
MHRA – Advanced Therapy Medicinal Product regulation. https://www.gov.uk/government/organisations/medicines-and-healthcare-products-regulatory-agency
Biovault Technical – Processing and storage pages. https://www.biovaulttechnical.co.uk/processing
PMC5629362 - JACIE accreditation for blood and marrow transplantation.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5629362/